Research Journal for Veterinary Practitioners


Review Article
Research Journal for Veterinary Practitioners 1 (3): 23 – 30Excretory Urography in Animals: a Review
Bashir Ahmed Moulvi, Jalal–ud–Din Parrah, Hakim Athar, Mohammad Moin Ansari*, Qayem Khan
-
Sher–e–Kashmir University of Agricultural Sciences and Technology of Kashmir, Faculty of Veterinary Sciences and animal Husbandry, Division of Veterinary Surgery & Radiology Shuhama, Alastaing, Srinagar–190006, J&K, India
*Corresponding author:[email protected]
ARTICLE CITATION:
Moulvi BA, Parrah JD, Athar H, Ansari MM and Khan Q (2013). Excretory urography in animals: a review. Res. j. vet. pract.. 1 (3): 23 – 30.
Received: 2013–07–06, Revised: 2013–08–01, Accepted: 2013–08–02
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/13/76/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The urinary system requires special attention for the expected increase in urinary problems associated with old age and due to its close association with genital organs. Excretory urography is indicated for a number of urogenital affections including colic, renal mass, renal haematoma, uroliths, trauma to the urinary tract, ureteral diseases, bladder affections like, congenital neurogenic bladder, postoperative urinary tract procedures etc. Excretory urography remains the first choice for the diagnosis of these affections, as it could not be replaced by the recently invented diagnostic techniques like ultrasonography. Excretory urography is considered better than ultrasonography because former technique unlike latter is considered a fairly accurate barometer of a total and relative function of the kidneys. Initial intravenous pyelography (IVP) has been modified by infusing large volumes of diluted contrast material over a prolonged period of time called Drip Infusion Pyelography (DIP) to avoid the use of abdominal compression and to make possible emergency urography without patient preparation. In order to comprehend the diagnostic utility of excretory urography all its aspects like patient preparation, dose and speed of injection of contrast medium, timing of post injection radiography besides brief history of radiology and contrast media are reviewed in this article.
INTRODUCTION
The lately discovered diagnostic techniques of imaging like ultrasonography could not replace the excretory urography. Instead, excretory urography has been found better than these techniques in the diagnosis of renal and other diseases. Michael et al. (1985) carried out prospective study in 61 patients to compare the diagnostic accuracy of sonography and excretory urography. Correct diagnosis was made by sonography in 66% and by urography in 85% cases. Urograms yield more information as they allow an estimation of renal function. In another prospective study conducted in 120 women with urinary tract infection, a good correlation was found between the two techniques in detecting hydronephrosis, calculi 5mm or more in size, major postpyelonephritis scarring, small cortical scars and slight calceal dilation. Calculi of 4 mm or less were detected better by intravenous urography than sonography (Aslaksen et al., 1990). About four million excretory urographic studies are done each year alone in the United States in medical practice at a total cost of more than a half million dollars (Rajindra, 1985). Having been able to retain its significance, despite the tremendous advancement made in diagnostic imaging techniques, excretory urography deserves to be reviewed in light of the innovations made in this technique.
A BRIEF HISTORY OF RADIOLOGY
X–rays were discovered on November 8, 1895 by Wilhem Conrad Roentgen, who received first Noble prize in physics in 1901, but veterinary profession received first official notice about the discovery through a reprint in The Veterinary Record in 1896 by Schuster (Williamson, 1998). Soon after the discovery of x–rays, the experiment was duplicated by various workers and, in March 1896, the first veterinary radiograph of an equine foot was published in The Veterinary Record by Paton and Duncan. Medical and veterinary radiology progressed very fast during early period, and soon after needles, bullets and other foreign materials were discovered radiographically. Dollar (of Dollar’s Surgery) published first practical and scientific article about Veterinary Radiology in 1896 in “The Veterinarian”. He stressed that soft tissue structures could not be differentiated (since contrast media were not developed by then). Motion unsharpness (blur) was a real problem because the exposure time for a human hand was 30–40 minutes. Therefore, veterinary radiologists were greatly disappointed. According to Prof. Eberlein, the limited use of x–rays by veterinary surgeons was because of three reasons: i) very long exposure time, ii) insufficient penetration of radiations, and iii) high cost of equipment (Williamson, 1998).
Today a radiologist wonders how the equipment used by pioneer workers produced x–rays. The equipment was run on battery connected to the primary of the coil. The primary was made and broken thousands of times in a minute to induce current in the secondary coil. The dim and flickering image in fluoroscopy was preferred to photographic image because of long exposure time and blurring produced on the radiograph. In The Veterinary Journal of 1896, it was reported that spreading of a fine layer of fluorescing substance, like fluospar, over the emulsion of photographic plate reduced the exposure time drastically from minutes to seconds, because, the emulsion was far more sensitive to the light emitted by the crystals under the influence of x–ray beam than to the beam itself. Thus the idea of intensifying screen was born (Williamson, 1998).
More technological development in the equipment started in 1920’s. The x–ray departments were supplied with alternating mains, enabling high–tension transformers to be used with improved radiographic results. However, the x–ray units were still not shock proof. In 1922, the old gas tubes were replaced by Cooledge hot cathode tube and double coated films replaced the old glass plates. Later, Potter–Bucky diaphragm was invented by Gustav Bucky to control scatter radiations. In 1928, the International Recommendations for Radiological Protection were published. Although radiologists knew them long before yet the radiation safety precautions were ignored. Veterinary Radiology, the first comprehensive textbook on small animal radiology/Radiography was published in 1944 by Gerry B. Schnelle of The Angel Memorial Hospital, Boston, USA. Then more books appeared in 1963.
A BRIEF HISTORY OF DEVELOPMENT OF CONTRAST MEDIA
It is very strange that none of the elements, from Mendeleev’s periodic table, other than iodine, has been found suitable as intravenous radiographic contrast agent. There are many elements with even higher atomic number and more radiopaque than iodine, but so far no other element has been found suitable to be injected safely intravenously in sufficient dose to produce diagnostic radiopacity. Contrast myelography using lipiodol (iodized poppy seed oil) was introduced by Sicard and Forester in 1921. Moinz tried the technique in cerebral circulation to localize intracranial tumours (Veiga–Pires and Grainger, 1982). He tried bromine and iodine salts of sodium, potassium, lithium, strontium and even rubidium in rabbits, monkeys and dogs, but all were too toxic to produce carotid angiogram. In 1929 he achieved a spectacular success in carotid angiography using thorium dioxide. Thorium dioxide had the beneficial properties essential to clinical angiography. It produced little acute intravenous toxicity, was almost painless on arterial injection and was intensely radiopaque. But after a few years thorium was banned as a diagnostic medium because it is a powerful emitter of µ–radiations (helium nuclei) and because of its long half–life of 1010 years, it is stored permanently in the body in reticulo–endothelial system, mainly liver, spleen and lymph node. The organ in which it is stored is continuously bombarded with µ–radiations to produce malignant tumors in 20–30 years.
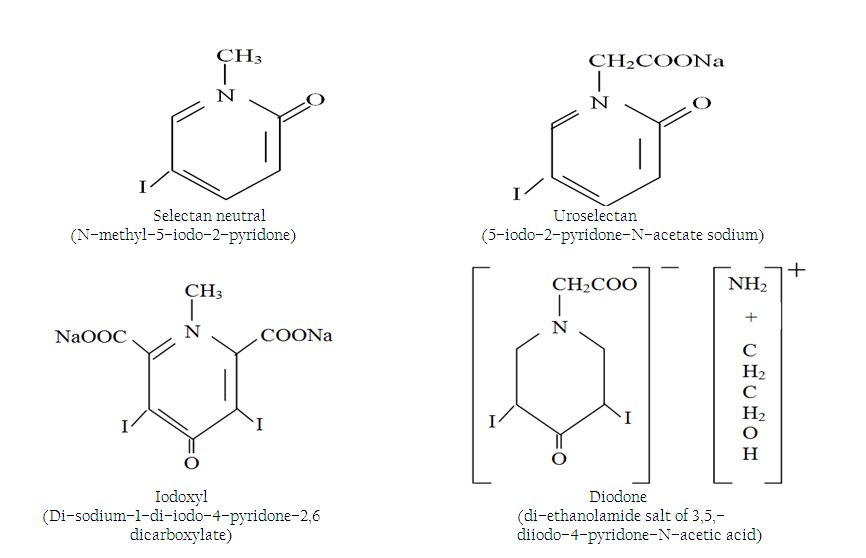
Incidentally it was observed that urine of some of the syphilis patients, who had been treated with large oral or intravenous dose of sodium iodide, was opaque to x–rays (Osborne et al., 1923). This was the first glimmering of successful visualization of urinary tract. But sodium iodide was too toxic to be used for radiographic purpose. Three years later, Professor of Chemistry, Arther Binz and his assistant, Curt Rath synthesized organic iodine preparations of pyridine. This was named as Selectan neutral. It was observed that the heterogeneous pridine ring had the extraordinary effect of detoxifying arsenic and iodine. Still selectan neutral was not suitable for clinical urography as the methyl group of selectan neutral was considered toxic. Therefore, this methyl group was changed to acetic acid and compound became 5–iodo–2–pyridone N–acetic acid, sodium salt of which was called Uroselectan (Binz, 1931). This was the first time the urinary tract was reliably visualized radiographically, apart from retrograde pyelography. Within two years of clinical introduction, uroselectan was superceded by two other improved pyridone products, namely Diodrast (Diodone) and Neo–iopax (Iodoxyl, Uroselectan B), both containing two iodine atoms instead of one atom in uroselectan. These two products were successfully used as radiographic contrast medium of choice for next 20 years.
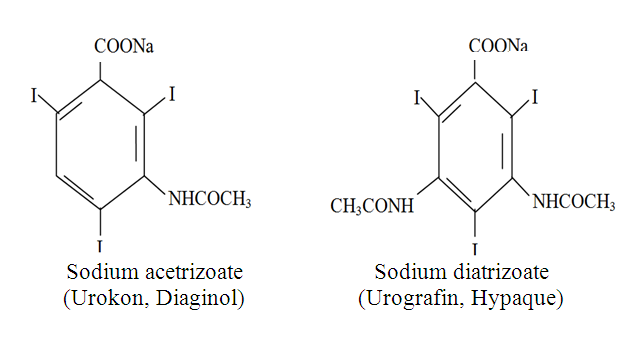
In 1933 Swick proposed the 6–carbon atom benzene ring as carrier of iodine instead of 5 carbon atom and 01 nitrogen atom heterocyclic pyridine ring, and thus sodium acetrizoate was introduced into clinical urology in 1952. In 1954 sodium diatrizoate was introduced as Urograhpin and Hypaque. This product and its immediate derivatives such as iothalamate (Conray), metrizoate (Triosil) are the standard contrast media now–a–days, injected intravenously every day in probably every x–ray department. Sodium iothalamate (70% w/v) solution (Conray–420) has been found an ideal contrast medium for excretory urography in dogs because of its safety, production of high quality urographs, delivery of high doses of iodine in minimal volume, low viscosity, low cost and easy availability (Parrah et al., 2001).
FIRST GENERATION LOW OSMOLAR CONTRAST MEDIA
The conventional contrast media are ionic monomeric salts of tri–iodinated substituted benzene ring. The toxic reactions of these contrast media are not because of chemical toxicity but because of high osmolality of the contrast media (about 2200 mosmol/kg water as against 300 mosmol/kg of body fluid).
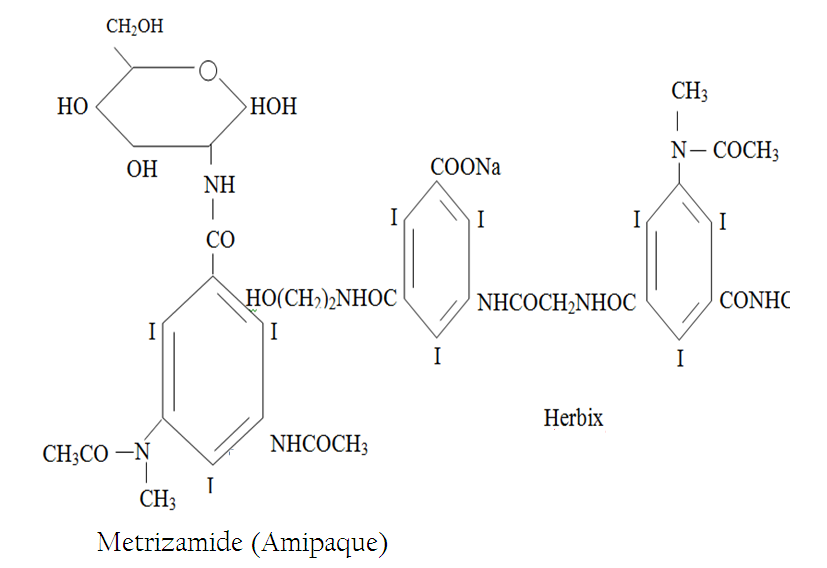
It was suggested that ionizing carboxyl group of this contrast media be transformed into non–dissociating amide group, that theoretically reduce the osmolality by 50% without any change in iodine contents (Almen, 1969). This led to the formation of non–ionic metrizamide (Amipaque) in 1974 (Dennis and Herrtage, 1989). This compound had iodine to osmotic particle ratio of 3:1 as against 3:2 for conventional contrast media. This contrast agent has revolutionized the clinical practice and diagnostic value of myelography.
SECOND GENERATION LOW OSMOLAR CONTRAST MEDIA
Metrizamide has a disadvantage that it cannot be sterilized by autoclaving and is available as freeze–dried lyophilized powder form and is therefore, very expensive. Modifications in the formula of metrizamide has produced second generation low osmolar contrast media e.g., iohexol (Omnipaque) and iopamidol (Neopam). These are stable in solution and can easily be sterilized by autoclaving. Therefore, they are cheaper than metrizamide but with the same iodine to osmotic particle ratio of 3:1. Furthermore, they are even less toxic than metrizamide. One more member of second–generation contrast media is ioglate (Herbix). It consists of two iodinated benzene rings forming a dimmer. Only one acid group is converted to non–dissociating group while the other ionizes in solution. It means that a molecule of ioglate contains six iodine atoms and in solution dissociates into two particles. So this compound also has the same iodine to osmotic particle ratio as other two compounds of the group. The osmolality of all these low osmolar contrast media is almost the same and about 1/3rd of the conventional contrast media at the same iodine concentration.
THIRD GENERATION LOW OSMOLAR CONTRAST MEDIA
The development of third generation low osmolar contrast media is in progress. Two compounds viz., iodixanol and iotrotan have already been produced. These are produced like ioglate but in these both of the acid groups are converted to non–ionic groups. So these dimmers are completely non–ionic and contain six iodine atoms per molecule giving iodine to osmotic particle ratio of 6:1.
EXCRETORY UROGRAPHY
The urinary system is the chief excretory system of the body. The kidneys play an important role in maintaining fluid and electrolyte homeostasis, control blood pressure and release hormonal agents (erythropoietin) into blood stream, which affects blood formation (Bloom and Fawcett, 1976). This system requires special attention for the expected increase in urinary problems associated with old age and due to its close association with genital system. Dogs suffer from many renal diseases. In a study, out of 7236 clinically ill dogs, 1000 (13.8%) suffered from renal diseases (Schepper, 1977).
Radiography is considered the first investigative tool after clinical examination. The radiographic study of urinary system, right from kidneys to urethra, can reveal many disease conditions not easily revealed by clinical examination. But the urinary tract, because of its deep seated location in the abdominal cavity and being of similar radiographic density to adjacent tissues, is not well visualized on plane radiograph. In order to visualize the details of these structures radiographically, one has to introduce a radio–opaque dye or contrast medium that outlines the structures of interest without invading other tissues. Excretory urography is a type of contrast study and thus a satisfactory anatomic tool (Parrah et al., 2002b) providing information regarding renal function and disease pathophysiology (Kneller, 1974; Osborne et al., 1972; Heuter, 2005). Furthermore nephrograms can be a valuable tool to make differential diagnosis of renal and extra–renal lesions (Weans and Flornece, 1947), besides, as a diagnostic aid for renal ischaemia (Siggers, 1961; Schwarz and Gleason, 1962 and Martin et al., 1963) and renal hydatid disease (Turqut et al., 2009).
TECHNIQUE
The contrast medium can be introduced into the urinary tract in two ways: i) instrumental method or retrograde pyelography or ascending pyelography, and ii) excretory method or intravenous pyelography (IVP).
Retrograde cystography and pyelography was first introduced by VonLichtenberg and Voelcker in 1905 using Kollargol (colloidal preparation of silver) (Grainger, 1982). In this case a radioopaque catheter is introduced into the ureters under cystoscopic control. Final position of the catheter is checked fluoroscopically and the contrast medium is introduced into the kidney through the catheter. This method gives excellent details even if the kidneys have ceased to function. The great disadvantage of this method is that the introduction of catheter is very difficult in large female dogs and almost impossible in small females or males even if cystoscope of suitable size is available. Also no information is obtained regarding function of the kidneys.
The excretory method relies on the normal functioning of the kidneys because all the modern excretory urographic contrast media are excreted by glomerular filtration (Grainger, 1972 and Talmer, 1972). In excretory urography the contrast medium is injected into convenient vein and a series of radiographs are taken. The kidneys and ureters are visualized by excretion of urine containing the contrast medium. Thus, the use of instruments and the associated risks are avoided. This method has various disadvantages including requirement of high concentration of contrast medium to obtain an adequate contrast in kidney region, occurrence of some toxic or allergic reactions, and loss of kidney details if its function is severely impaired (Bishop, 1953).
Patient Preparation
Patient preparation is the first pre–requisite vis–a–vis the diagnostic urography (Singh et al., 1977 and Parrah et al., 2002a). Food and water should be withheld for 12 hours before examination. The bowel should be evacuated by means of an enema just before the patient is taken to the x–ray room. This avoids superimposition of urinary organs with gas, food and faecal matter present in the alimentary structures. Visualization of these structures can also be improved by insufflation of abdominal cavity and also by compression of ureters. However, these procedures are reported to cause deviation of kidneys and ureters to some extent (Singh et al., 1977 and Parrah et al., 2002a). Anaesthesia is desirable because the animal is to be restrained in dorsal recumbency for about an hour. First a lateral plan radiograph of the kidney region should be taken and then the patient should be restrained in dorsal recumbency and a plan radiograph should be taken and processed and examined to ascertain that i) abdomen is free from gas and faecal matter, ii) suitable exposure factors for individual patient and proposed examination, and iii) pad and compression devices, if used, do not cause undesirable shadow. The contrast medium should now be administered through a convenient vein i.e. cephalic or saphenous. Initially 1–2 ml should be injected and 30–40 second should be allowed to elapse. This enables observation of undesirable reaction, if any. If no reaction occurs, the remainder of the contrast medium should be injected rapidly. The time should be noted at the start of injection and this forms the reference point for all subsequent films. Radiographs should be taken in ventro–dorsal or lateral views at different intervals for study of different structures of the urinary system. However, the right lateral view is usually preferred because it allows for the most longitudinal separation of the right and left kidneys (Heuter, 2005).
Dehydration
The urographic contrast media, particularly the trio–iodinatede compounds, commonly used these days are filtered by glomerulus without any tubular reabsorption or secretion (Woodruf and Malvin, 1960). Rather, the contrast medium is concentrated in the tubules by reabsorption of water. For the purpose of maximum tubular reabsorption of water, the patients are dehydrated by overnight fluid restriction, before examination. But restriction of fluid has been stated to have little or no effect on nephrogram (
Dure–Smith, 1976) although overnight fluid restriction may cause slight increase in pyelographic density due to concentration of contrast media, but this is of no significance (
Dure–Smith, 1966 and 1976 and Cattell et al., 1967). In uraemic patients dehydration is not only undesirable, but it is unlikely to cause concentration of contrast media in tubules (
Dure–Smith, 1966). Also in patients with renal failure, fluid restriction can be dangerous (Grainger, 1972) and thus should be avoided in such conditions (Brown et al., 1970). In babies, a serious degree of dehydration may result, if they are first dehydrated and then given high dose of contrast media, producing marked diuresis (Powell et al., 1967). This can be true in veterinary practice also.
Abdominal Compression
The non–significant effect of dehydration on the excretory urograms is because of poor filling of upper collecting system. Therefore, abdominal compression is applied to obstruct ureters. However, it is often ineffective in occluding ureters. Furthermore, it is uncomfortable to the patient and sometimes it cannot be tolerated because of pain or tenderness e.g., after laparotomy. Under some circumstances, it can be dangerous e.g., when there is suspicion of ruptured kidneys (
Dure–Smith, 1966). However, in one study conducted on mongrel dogs the role of compression bandaging in obtaining the diagnostic urographs was found equally important for both the techniques of urography without causing any inconvenience to the animals (Parrah, 2002).
Anaesthesia
Most of the animals with urinary distress are of questionable anaesthetic risk. In one study best results were obtained when two attendants restrained the dog, without anaesthesia, while taking radiographs (Tennille and Thronton, 1958). However, some physical reactions were observed following injection of contrast media. These included nausea, vomiting, flushing of skin, urticaria like lesions and vertigo like seizures. These reactions depended mostly on the individual animal and to a lesser extent on contrast media used or its concentration. Extravasation of contrast media during injection causes slight pain at the time and moderate swelling of the area the next day, which subsides by 48 hours (Parrah et al., 2001). However, trivial reactions recorded in other studies were not observed during a study conducted on apparently healthy mongrel dogs following the general anesthesia for conducting urography (Parrah et al., 2002a).
Dose of Contrast Media
Number of iodine atoms per molecule is important in producing good nephrogram. Various workers have compared different contrast media used for intravenous pyelography in humans (Nicolai and Humphries, 1957), cat (Harrod and Frost, 1955) and dog (Tennille and Thronton, 1958) and found that contrast media with three iodine atoms per molecule produced better nephrograms than contrast media with only two atoms per molecule. Besides, dose of contrast medium also plays an important role in density of excretory urogram. Increasing the dose of contrast medium, to a certain limit, increases the density and thus visualization of urinary structures. In a study, increasing the dose of contrast medium from 200 mg to 400 mg iodine per 0.45 kg body weight had significant effect on radiographic density of various structures. But a dose of 800 mg iodine per 0.45 kg body weight did not increase the percentage of animals in which various structures could be visualized, however, it only increased the time over which these structures could be visualized (Feeney et al., 1979). It is therefore, recommendable that 400 mg iodine per 0.45 kg body weight as sodium salt of tri–iodinated contrast media be administered rapidly intravenously for obtaining urograms for adequate density (Parrah et al., 2002b).
Duration of Injection
The speed with which the injection of contrast medium is made influences the opacity of the urinary structures on an excretory urogram. Numerous investigators have tried to develop a practical and safe clinical method of obtaining nephrograms of sufficient density to be of diagnostic value. The concept of rapid intravenous injection of contrast organic iodine solution for the production of dense nephrograms was introduced for the first time in1938. However, the first paper based on this concept was published in 1947 by Weans and Florence. Weans et al. (1951) and Vesey et al. (1950) injected 50 ml iodopyroset (diodrast 70%) in two seconds period and obtained satisfactory nephrograms 9–12 seconds post–injection in 83% cases. Wall and Rose (1951) injected sodium acetrizoate in five seconds and took radiographs at 10–25 seconds post–injection. They obtained opacification of renal parenchyma in 100% cases. Wald (1956) obtained only 64% good nephrograms by injecting 24 ml sodium acetrizoate in 10–15 seconds and making radiographs 30 seconds after injection. Schwartz and Gleason (1962) injected 30 ml sodium diatrizoate (Hypaque 50%) in 121 seconds. They concluded that one radiograph immediately after completion of injection and other two minutes later offer best chances of obtaining nephrographic effect. They reported that reducing the injection time to 30 – 40 seconds produced even denser nephrograms. Thus it seems that nephrographic effects can apparently be obtained by various alterations of an excretory urogram with minimum of side effects and/or inconveniences to the patient. Rapid injection does not produce higher percentage of reactions than are noted with slow injection. Therefore, the reluctance to give rapid injections is not probably sound (Weaver and Yelderman, 1966).
Glomerular Filtration Rate
Osmotic diuretic effect of contrast media (Lasser et al., 1975 and Dure–Smith, 1970) results in increased urine volume which in turn causes volume distension of various urinary structures (Droph et al., 1977). Because all the urographic contrast media are excreted by glomerular filtration (Talmer, 1972 and Grainger, 1972), glomrular filtration rate may influence the visualization of different structures during excretory urography. In a study the appearance of kidney was found unrelated to the glomerular filtration rate in dogs with induced renal disease (Feeney et al., 1980). In another report, glomerular filtration rate in man has been stated to have little effect on excretory urogram when glomerular filtration rate is 50% or more of the normal (Cattell et al., 1967). In dogs with spontaneous renal disease, quality of excretory urogram has been found to be affected inversely with magnitude of serum urea nitrogen (Brown et al., 1970).
Time of Radiography
Timing of post–injection radiographs has a good bearing on the achievement of dense and diagnostic urographs (Parrah et al., 2003b). Radiographs should therefore be taken when structures are of maximum size or density or both. Feeney et al. (1979) consistently observed that visualization of kidney immediately or 5 minutes post–injection; renal pelvis at 10 and 20 minutes; pelvic diverticula at 40 minutes and ureters at 5, 10 and 20 minutes after injection of contrast medium. They obtained maximum measurement for kidney at 5 and 10 minutes, renal pelvis at 40 minutes and ureters at 5 minutes after injection. Based on these observations they concluded that radiographs of greater value are those taken immediately and at 5, 20 and 40 minutes post–injection. However, Parrah et al. (2003b) observed that post–injection exposures from 10 – 15 and 20 minutes were useful for delineation of urinary tract organs.
ADVERSE EFFECTS OF CONTRAST MEDIA
The manufacturers of contrast media warn that some dangerous side effects may be encountered by the use of these contrast media. Because of high atomic number, iodine is toxic in different degree in different forms. In one study, Moga et al. (1972), on the basis of estimation of blood urea nitrogen and urine analysis, observed that both Conray–420 and Diaginol were toxic to renal system. Also the toxicity was more with former. However, the toxicity was non–clinical and within tolerable limits. On the other hand various other workers (Borthwick and Robbvie, 1969; 1971 and Singh et al., 1977) did not observe toxicity to iodine in any of the contrast media used (Conray–420, Conray–280, Diaginol) up to 72 hours post–injection. Most serious of the side effects is allergy to iodine. However, majority of side effects come under unpleasant sensation rather than actual hazards and depend mostly upon the individual animal than upon contrast medium itself (Tennille and Thronton, 1958). If the animal is anaesthetized, these side effects are minimized (Bishop, 1953 and Parrah et al., 2001). Almen (1969) postulated that toxicity of contrast media is not due to its chemotoxicity but due to hypertonicity of the solution.
EVALUATION OF UROGRAPH
The urographs are usually evaluated in terms of alterations in location, radiodensity, shape and size of the urinary tract organs. The phases of the excretory urograms are the nephrographic and pyelographic phases. The nephrogram is seen as the opacification of the functional renal parenchyma, whereas the pyelogram is the opacification of the renal pelvis, pelvic recesses and ureters (Feeney and Johnson, 1997; Biery, 1978). Nephrograms are classified as good, fair and poor (Weaver and Yelderman 1966). Radiographs with brightly opacified renal parenchyma and good to excellent delineation of renal outline are graded as ‘good’. These nephrograms are of definite diagnostic value. Nephrograms with definite opacification of renal parenchyma and moderately clear delineation of renal outline are graded ‘fair’. These are also of some diagnostic value. Those with slight or no opacification of renal parenchyma and failure to demonstrate renal outline are graded ‘poor’. These are considered to be of no diagnostic value.
The kidneys in dogs and cats are located in retroperitoneal space in association with the last thoracic and first three or fourth lumbar vertebrae. The right kidney is located more cranial than the left. The shape of kidney in both species is somewhat elongated, resembling a bean and with the hilus directed medioventrally (Parrah et al., 2002b). In general the dog kidney is approximately three times the length of L2 as visualized on the ventrodorsal view (Parrah et al., 2000b), while in cat; the most accepted renal length is 2.4 to 3 times the length of the L2 vertebral body (Feeney and Johnson, 1997). The renal pelvis, and pelvic recesses (pelvic diverticula) in the dog does not exceed 2 or 3 mm in diameter (Feeney and Johnson, 1997). The ureters are primary retropertoneal but become intraperitoneal as they approach their termination at the bladder trigone. The size of each ureter is usually less than 2–3 mm in diameter as they exit the kidney. Ajadi et al. (2006) performed three series of trials involving 10 domestic short–haired cats to determine the influence of dosage of contrast media or type of chemical restraint on feline excretory urography. It was therefore concluded that increasing the dosage of urografin above 800 mg/kg in cats does not provide additional beneficial effects on the nephrograms produced. Xylazine sedation was observed to produce better nephrographic opacification, however, with delayed nephrographic fading compared to ketamine sedation.
DIAGNOSTIC UTILITY OF EXCRETORY UROGRAPHY
Both congenital (Webb, 1974), as well as acquired pathological conditions viz. inflammatory (Ganesh et al., 1995), neoplastic (Widmer and Carlton 1990; Sterman et al., 1990) and obstructive (Walker and Douglas, 1970; Zontine, 1975) diseases affecting kidneys, ureter and urinary bladder are clearly appreciated on excretory urograms. Focal, non uniform opacification may be caused by a neoplasm, haematoma, cyst, infract, hydronephrosis and abscess. Non opacifiction may occur with renal apalsia, renal artery obstruction, nephrectomy or non functional renal tissue and insufficient or extravascular contrast media injection. Pyelonephritis can be diagnosed by pelvic dilation, proximal ureteral dilation and absent or incomplete filling of the pelvic diverticuli. Hydronephrosis will present with dilation of renal pelvis, diverticuli and ureter. Uroliths and blood clots present as filling defect in the renal pelvis. Ectopic ureters and uretral duplication may have same radiographic presentation (Feeney and Johnson, 1997; Biery1978). Ureterocele or diverticulum can be appreciated as a focally enlarged ureter with regular shape (Stiffler et al., 2002). A reproducible filling defect in the contrast medium in the ureter may be caused by a calculus, neoplasm or stricture (Feeney and Johnson, 1997; Biery, 1978). Veshkini et al. (2011) performed the experiment to evaluate the feasibility of subcutaneous injection of iodixanol in providing a safe and diagnostic urogram in twelve clinically healthy adult Persian squirrels. It is concluded that subcutaneous urography is an effective and reliable method for urography studies in squirrel except for nephrogram.
Drip Infusion Pyelography (Dip)
Another method of excretory urography is by injecting a large volume of contrast solution of low concentration by drip infusion over a large period of time. This procedure was first reported in man by Schanker in 1964 and subsequently by (Harris and Harris, 1964 and Collins, 1966). Each of these workers gave a different name to the technique e.g., ‘Drip Infusion Pyelography’ (Schanker, 1964), ‘Infusion Urography’ and ‘Saturated Pyelography’ (Collins, 1966). Of these ‘Drip Infusion Pyelography’ became popular and
Wendth (1965) stressed that this technique should be termed by its initials ‘DIP’ just as standard intravenous pyelography is termed ‘IVP’ to differentiate the two procedures. Evans and Knoblaugh (1970) used 300 ml of contrast solution (150 ml of 50% Hypaque and 150 ml of 5% glucose) dripped intravenously as quickly as possible through an 18 guage needle. However, Schanker (1966) suggested that a 120 + 120 mixture gives optimal results in an average patient. They did not use any preparation for the examination. They preferred the patient to be ambulatory. Solid food was withheld only for four hours. Films were exposed at the completion of infusion and 5 and10 minutes later. Evans and Knoblaugh (1970) reported certain problems with DIP. For example, it does not indicate status of renal function nor does it indicate amount of residual urine in the bladder. As excellent films are produced which reduce the need of additional cystography or retrograde pyleography, thereby eliminating the possibility of occasional discovery of an asymptomatic lesion of the urethra, prostate or bladder. However, advantages are manifold. Preparation of the patient in terms of dehydration or fasting is not required.
Abdominal compression applied for ureteral filling is not required thus avoids discomfort to the patient or deviation of ureters and bladder. This enables evaluation of the urinary tract in its normal physiologic state of hydration, as dehydration is not required for the procedure. It causes excellent filling of kidney structures thus number, shape, position and size of renal parenchyma are accurately ascertained (Evans and Knoblaugh, 1970). However in other studies conducted on dogs, abdominal compression and other patient preparatory measures, especially withholding food and water were found equally important for obtaining good urograms with both the techniques of excretory urography i.e., IVP and DIP ( Parrah, 2002; Parrah et al. 2003a). Moreover it is reported that good radiographs are obtained in cases of chronic renal failure or when conventional IVP does not give adequate films (Borthwick and Robbvie, 1969), and also in human patients with high blood urea levels (Schander, 1964). As already stated the intravenous urographic contrast media have some side effects. These effects can be reduced by using DIP. However, no complication that can be attributed to DIP has been observed. Allergic reactions with DIP were not observed even when IVP and DIP were performed on the same patient on the same day or 24–48 hours later. Patients who experienced mild response to IVP did not react to DIP (Harris and Harris, 1964). This supports the postulation of Almen (1969) that the toxicity is due to hypertonicity of the contrast medium. In DIP, contrast is used in very low concentration that reduces the tonicity of the solution injected. This is the reason for lower toxicity of contrast media in DIP.
SPECIFIC VALUES OF DIP
Evans and Knoblaugh (1970) have enumerated some specific values of DIP. These include:
- Emergency urography: Because prior preparation of the patient for DIP is not necessary, it becomes a ready to use procedure for emergency situations like ureteral colic and trauma. Upper urinary tract obstruction, particularly marginally significant obstruction, can be evaluated by DIP at the time of normal or maximal rate of urine drainage
- Urinary tract trauma: In case of renal trauma, complete or partial absence of nephrogram indicates main renal artery or branch artery interruption. Similarly extravasation of contrast media from the pelvis, ureters, bladder or urethra during opacification of these organs indicates rupture of specific conduit. Renal dislocation by haematoma or uroma is more readily assessable by DIP than by IVP.
- Uraemia: DIP can be effective in evaluating urinary collecting system even in patients with a creatinine clearance as low as 20 ml/min.
- CineRadiography: As DIP provides excellent contrast, peristaltic activity of renal pelvis; ureteropelvic area and ureters can be recorded on film. CineRadiography of neuromuscular activity of the detrusor muscle, vesical neck and external sphincter can be recorded as part of DIP.
Dure–Smith (1966) summarizes the following advantages and disadvantages:
ADVANTAGES
Dense nephrograms: Dense nephrogram is obtained for better demonstration of renal parenchyma; Visualisation of whole ureters: By DIP whole of the ureters is visualized and thus higher proportion of ureteral affections can be diagnosed; Hydronephrosis: Because of more volume of contrast media and larger diuresis, the dilated system is outlined more quickly and satisfactorily; Absence of dehydration: Because dehydration is not required, emergency urogram can be done; Absence of ureteral compression:–Uncomfortable, unreliable, not possible in post–laparotomy, dangerous in ruptured kidney; Uraemia; Avoids retrograde urography.
DISADVANTAGES
Denser nephrograms obscure calcycal details; unreliable as a test of residual urine and increased cost. Finally, as the contrast media used for DIP are the same as those used for IVP, therefore, the contra–indications are also the same such as poor kidney function or idiosyncrasy or allergy to iodine (Collins, 1966).
CONCLUSION
Though newer techniques of imaging are continuously invented with their rapid innovations, still excretory urography has been able to retain its paramount significance in the diagnosis of urinary tract diseases, especially with regard to kidney function. However a very little work has been conducted in domestic animals, which desires immediate attention for establishing the protocol for its immediate use, especially in the dairy animals and horses, whose cost have witnessed unprecedented rise over the past few decades.
REFERENCES
Ackerman N (1974b). Intravenous pyelography. J. Am. Ani. Hosp. Assoc. 10: 281-84.
Ajadi RA, Adetunji A, Omoerah VO and Okoh, JU (2006). Influence of dosage and chemical restraints on feline excretory urography. J South African Vet. Assoc. 77: 202-204.
PMid:17458345
Almen T (1969). Contrast agent design. Some aspects of the osmolality. J. Theoretical Biol. 24: 216-26.
http://dx.doi.org/10.1016/S0022-5193(69)80047-0
Aslaksen A, Baerhein A, Hunskaar S and Gothlin JH (1990). Intravenous urography versus ultrasonograophy in evaluation of women with recurrent urinary tract infection. Scan. J. Prin. Health Care. 8: 85-89.
http://dx.doi.org/10.3109/02813439008994936
PMid:2218159
Biery DN (1978). Upper urinary tract, in Obrein TR (ed): Radiographic diagnosis of abdominal disorders in the dog and cat, Philadelphia, P A Saunders, pp. 481-542.
Binz A (1931). The chemistry of uroselectan. J. Urol. 25: 297-301.
Bishop EJ (1953). A method of visualizing the urinary tract and a basis for assessing renal function in small animal. Radiography. J. Am. Vet. Med. Assoc. 123: 187-92.
PMid:13084481
Bloom W and Fawcett DW (1976). A Textbook of Histology. 10th Edn., Asian Education. Igaku Shoin Ltd., Tokyo. pp 776, 782.
Borthwick R and Robbie B (1969). Urography in dog by an intravenous transfusion technique. J. Small Am. Pract.10: 465 – 70.
http://dx.doi.org/10.1111/j.1748-5827.1969.tb04057.x
PMid:5387869
Borthwick R and Robbie B (1971). Large volume urography in the cat. J. Small Am. Pract. 12: 579-83.
http://dx.doi.org/10.1111/j.1748-5827.1971.tb06178.x
PMid:5166211
Brown CB, Gancy JJ and Fry IR (1970). High dose excretion urography in oliguric renal failure. Lancet. 2: 952 -955.
http://dx.doi.org/10.1016/S0140-6736(70)92128-8
Cattell WR, Fry IK and Spencer AG (1967). Excretion urography. (Part 1 and 2). Br. J. Radiol.40: 561-80.
http://dx.doi.org/10.1259/0007-1285-40-476-561
PMid:4952292
Collins V (1966). A technique for infusion urography. Radiography. 32: 103 – 108.
Dennis R and Herrtage ME (1989). Low osmolar contrast media. Vet. Radiol. 30: 2-12.
http://dx.doi.org/10.1111/j.1740-8261.1989.tb00746.x
Droph S, Sovak M and Talner LB (1977). Why does kidney size change during intravenous urography? Invest. Radiol.12: 246 – 50.
http://dx.doi.org/10.1097/00004424-197705000-00007
Dure-Smith P (1966). Drip infusion and routine urography: a comparative trial. Br. J. Radiol.39: 655-661.
http://dx.doi.org/10.1259/0007-1285-39-465-655
PMid:5920123
Dure-Smith P (1970). The dose of contrast medium I intravenous urography: A physiologic assessment. Am. J. Roentgenol.108: 691-697.
http://dx.doi.org/10.2214/ajr.108.4.691
Dure-Smith P (1976). Fluid restriction before excretory urography. Radiology. 118: 487-489.
http://dx.doi.org/10.1148/118.2.487
PMid:1250993
Evans AT and Knoblaugh RA (1970). Routine drip infusion pyelography. Am. J. Surg. 119: 655 – 659.
http://dx.doi.org/10.1016/0002-9610(70)90236-9
Feeney DA and Johnson GR (1997). The kidneys and ureters, In Thrall DE (ed). Textbook of veterinary diagnostic radiology (ed 3), Philadelphia, PA, Saunders, pp466-478.
Feeney DA, Thrall DE, Barber DL, Curvar DH and Lewis RE (1979). Canine excretory urogram: effect of dose, time, and individual dose variation. Am. J. Vet. Res. 40: 1596-1604.
PMid:525879
Ganesh TN, Balasubramini NN and Dewan Muthu Mhammed MS (1995) Radiographic contrast studies of the urinary tract in four dogs: a clinical report. Indian J.Vet. Sur. 16: 59-61.
Grainger RC (1972). Renal toxicity of radiological contrast media. Br. Med. Bull. 28: 191-195.
PMid:4569777
Grainger RC (1982). Intravenous contrast media – the past, the present and the uture. Br. J. Radiol. 55: 1-18.
http://dx.doi.org/10.1259/0007-1285-55-649-1
PMid:7032636
Harris JH and Harris JH (1964). Infusion urography. Am. J. Roentgenol .92: 1391.
Harrod EM and Frost RC (1955). Hypaque, a new urographic contrast media. Vet.Rec. 67: 671.
Heuter KJ (2005). Excretory urography. Clin. Tech. Small Anim. Pract. 20: 39-45.
http://dx.doi.org/10.1053/j.ctsap.2004.12.006
PMid:15822529
Kerk H (1932). X-ray in small animal practice. Vet.Rec.12: 171.
Kneller SK (1974). Role of the excretory urogram in the diagnosis of renal and ureteral diseases. Vet. Clin. North Am. 4: 843-861. PMid:4479909
Lasser FC, Lang JH and Hanblin AE (1975). Contrast and electrolyte diagnosis of the intravenous pyelograqm (Part 1 & 2). Invest. Radiol.10: 300-313.
http://dx.doi.org/10.1097/00004424-197507000-00003
PMid:241732
Martin JF, Deyton WE and Glenn JF (1963). The minute sequence pyelogram. Am. J. Roentgenol.90: 55-62.
Michael CH, Jefrey IR, John GM and Charles AF (1985). Sonography vs. excretory urography in acute flank pain. Am. J. Roentgenol. 144: 1235-1238.
http://dx.doi.org/10.2214/ajr.144.6.1235
PMid:3890487
Moga IV, Angelo SJ and Das SC (1972). Observations on experimental pyelography in canines. Indian Vet. J. 49: 305-313.
Nicolai CH and Humphries CF (1957). A comparative study of the intravenous urographic media by the random selection technique. Am. J. Roentgenol.78: 106.
Osborne CA, Low DG and Finco DR (1972). Canine and feline urology. Philadelphia, WB. Saunders Co. pp 85-106.
Osborne ED, Sutherland CG, Scholl AJ Jr and Rowntree LG (1923). Roentgenography of the urinary tract during excretion of sodium iodide. J. Am. Med. Assoc. 80: 368-373.
http://dx.doi.org/10.1001/jama.1923.02640330004002
Parrah JD (2002). A comparative study on intravenous and drip infusion pyelography with and without abdominal compression in dogs. SKUAST. J. Res. 4: 45 – 50.
Parrah JD, Chowdhary, RJ and Gahlot, TK (2001). Sodium iothalamate 70% w/v solution-an ideal contrast medium for excretory urography in dogs. Intas Polivet. 2: 74 – 78.
Parrah JD, Chowdhary RJ and Gahlot TK (2002a). Preparation of the patient first pre-requisite vis-à-vis the diagnostic excretory urography in dogs. J. Applied Biol. Res. 4: 17-22.
Parrah JD, Chowdhary RJ and Gahlot TK (2003b). Pattern of excretion of the contrast medium from upper urinary tract of do during drip infusion pyelography-an experimental study. SKUAST. J. Res. 5: 39-44.
Parrah JD, Chowdhary RJ, Gahlot TK and Sharma CK (2002b). Radiographic anatomy of upper urinary tract in dogs. Indian J. Vet. Surg. 23: 86-80.
Parrah JD, Chowdhary RJ, Gahlot TK and Sharma CK (2003a). Drip infusion pyelography and routine pyelography- a comparative study in dog. Vet. Pract. 4: 7-12.
Powel T, Lentle BC, Dew B, et al (1967). Intravenous pyelography -a comparative trial of ten methods in patients with good renal function. Br. J. Radiol.40: 30-37.
http://dx.doi.org/10.1259/0007-1285-40-469-30
Rajindra K and Melyn HS (1985). The changing indication for excretory urography. J. Am. Med. Assoc. 254: 403-405.
http://dx.doi.org/10.1001/jama.1985.03360030093030
http://dx.doi.org/10.1001/jama.254.3.403
Schanker B (1964). Drip infusion pyelography: Indications and applications in urologic roetngen diagnosis. Radiology. 8: 12.
http://dx.doi.org/10.1148/83.1.12
PMid:14191647
Schanker B. (1966) Further experience with drip infusion pyelography. Radiology. 8: 34.
Schepper JDe (1977). Renal diseases in the dog. One thousand clinical cases. Vlaams Deirgenees Kundig Tijdschriff. 46: 18-25 (Vet. Bull. 47: 5710).
Schwarz GS and Gleason DM (1962). The time of maximum nephrogram effect in excretory urography. J. Urol. 88: 841-843.
PMid:13987422
Siggers RL (1961). Early physiologic nephrography as a test of kidney function. Radiology. 77: 452-457.
http://dx.doi.org/10.1148/77.3.452
Singh H, Kumar A and Pandiya SC (1977). Visualization of urinary tract in the dog using different contrast media and techniques. Indian Vet. J. 54: 139-143.
Sterman FA, Iwasaki M, Matera JM, Araujo NS-de and De Araujo NS (1990). What is your diagnosis? [Invasive papilliferous carcinoma in dog]. J. Am. Vet. Med. Assoc. 197: 511-512
PMid:2211299
Stiffler KS, Stevenson MA and Mahaffey MB (2002). Intravesical ureterocele with concurrent renal dysfunction in a dog: A case report and proposed classification system. J. Am. Ani. Hosp. Assoc. 38: 33-39.
PMid:11808543
Talmer LB (1972). Urographic contrast media in uremia-physiology and pharmacology. Radiol. Clin. North Am. 10: 421-432.
Tennille NB and Thronton, GW (1958). Intravenousurographic studies in the unanesthetized dog. Vet. Med. 53: 29 -40.
Turqut AT, Odev K, Kabaalioglu A, Bhatt S and Dogra VS (2009). Multitechnique evaluation of renal hydatid disease. Am. J. Roentgenl. 192: 462-467.
http://dx.doi.org/10.2214/AJR.08.1129
PMid:19155411
Veiga-Pires JA and Grainger RG (1982). The Portuguese pioneers of Angiography (MTP Press, Lancester, UK/Boston, USA).
Vesey I, Botter CT and Steinberg I (1950). Nephrography: Simplified technique. Radiol. 55: 827-833.
http://dx.doi.org/10.1148/55.6.827
PMid:14786421
Veshkini A, Tavana M, Haghdost IS, Masouleh MN and Savojbolaghi SH (2011). Excretory urography by subcutaneous injection of iodixanol in Persian squirrel (Sciurus anomalous). Pakistan Vet J. 31: 17-22.
Wald AM (1956). Nephrography during routine excretory urography. J. Urol. I75: 572-577.
Walker RG and Douglas SW (1970). The use of contrast media in the diagnosis of urinary tract abnormalities in the dog, with particular reference to infusion urography: a report of two cases. Vet. Rec. 87: 287 – 290.
http://dx.doi.org/10.1136/vr.87.10.287
PMid:5528574
Wall B and Rose DK (1951). The clinical intravenous pyelogram: Preliminary report. J. Urol. 66: 305-311.
PMid:14861959
Weans HS and Florence TJ (1947). Nephrography. Am. J. Roentgenol. 57: 338-541.
Weans HS, Olnick HM, James DF and Warren JV (1951). Intravenous nephrography: A method of toentgen visualization of kidney. Am. J. Roentgenol.65: 411-414.
Weaver RG and Yelderman JJ (1966). Production of nephrograms in excretory urography. J. Urol. 96: 971-975.
PMid:5956785
Webb AA (1974). Renal ectopic in a dog. Aust. Vet. J. 50: 519
http://dx.doi.org/10.1111/j.1751-0813.1974.tb14059.x
Wendth AJ Jr (1965). Infusion pyelography. Am. J. Roentgenol.95: 269.
http://dx.doi.org/10.2214/ajr.95.2.269
Widmer WR and Carlton WW (1990). Persistent haematuria in a dog with renal haemangioma. J. Am. Vet. Med. Assoc. 197: 237 – 232
PMid:2384325
Williamson HD (1998). Veterinary Radiology: history, equipment, technique, in diagnosis, protection practice. Vet.Rec.103: 84-87.
http://dx.doi.org/10.1148/radiology.207.1.152
http://dx.doi.org/10.1148/radiology.209.3.9844647
http://dx.doi.org/10.1148/radiology.206.2.9457176
PMid:9457176
Woodruff MW and Malvin RL (1960). Localization of renal contrast media excretion by stop flow analysis. J. Urol. 84: 677.
PMid:13786561